The False Promise of Healthcare as “Management”
We live in a medical culture that is content with management rather than cures. The Medical-Industrial Complex—an interwoven system of hospitals, pharmaceutical companies, insurers, government agencies, and universities—has built a fortress around the idea that being perpetually treated is the same as being healthy.
But treatment is not restoration. Management is not cure.
In fact, much of what passes as healthcare today is better named sick care: a system that sustains itself by maintaining patients in cycles of dependency rather than liberating them into wellness.
The Embarrassment of “First, Do No Harm”
Medicine’s foundational oath—first, do no harm—has been twisted into a bitter irony.
In 2000, Dr. Barbara Starfield published in JAMA that iatrogenic deaths (deaths caused by medical care itself: errors, adverse drug reactions, hospital infections, unnecessary surgeries) accounted for ~225,000 U.S. deaths annually, making medicine the third leading cause of death.
In 2016, Johns Hopkins researchers Martin Makary and Michael Daniel updated that figure to over 250,000 deaths per year (BMJ), still ranking third behind heart disease and cancer.
These are not rare and isolated events. They are systemic where patterns repeat themselves, and are built into the structure of the system itself.
Even the Hippocratic ideal has been inverted. Harm is not the exception—it has become the expectation, justified under the banner of “standard of care.”
Then there is the long list of side effects warning that the “cure” may, in fact, be worse than the condition. Small print pharmaceutical inserts and rushed explanations mask the reality: dizziness, fatigue, organ damage, dependency, even death. What should be an assurance of healing often reads more like a catalogue of new ailments waiting to be triggered. Patients are left to gamble—accepting harm as the price of “care,” while the system calls it progress.
If a side effect occurs, it no longer remains a “side” effect at all. It becomes a direct effect—an undeniable new condition that demands its own assortment of medications, each with their own cascading risks. Thus, the cycle continues: one prescription spawning another, one “treatment” birthing a fresh dependency, until the patient is buried beneath a daily fistful of pills rather than lifted into health.
Collateral damage is status quo—woven so deeply into the system that it’s normalized, excused, and even budgeted for. What should be rare and shocking is treated as inevitable, the “cost of doing business” in modern medicine. Patients pay that cost with their bodies, their trust, and too often their lives, while the system marches on as if harm were an acceptable companion to healing.
COVID-19 and the Collapse of Trust
If there was any remaining doubt about the fragility of trust in the medical system, COVID-19 exposed it.
A 2024 JAMA Network Open study (Perlis et al.) found trust in U.S. physicians and hospitals dropped from 71.5% in April 2020 to 40.1% in January 2024.
The American Board of Internal Medicine/NORC 2021 survey showed that while people trusted individual clinicians (84% trusted their personal doctor), institutional trust was dramatically lower (hospitals: 72%, the broader system: far less). Even physicians themselves only trust health care leaders and executives either completely or somewhat at a 66% rate.
The highest trust is relational and personal, but institutional trust is more fragile. A recent pandemic exposed how crises accentuate vulnerabilities. And generally, trust in organizational leadership and institutional bodies (e.g. health systems, government agencies like the CDC and the FDA) declined for many.
A door lock either works or it doesn’t—there’s no margin for error. That clarity has allowed a few trusted door lock companies to dominate the market for decades, because reliability is non-negotiable in this field. Medicine once carried that same kind of trust: people assumed the system would safeguard their health. But unlike a lock, where failure means a broken door or an invading intruder, failure in health care means broken lives. When the medical gatekeepers compromise reliability—whether through preventable errors, profit-driven choices, or eroded transparency—the cost is immeasurably higher. Trust, once lost, is not easily repaired.
The system’s heavy-handed messaging, contradictory protocols, and perceived alignment with pharmaceutical profits created a rupture. Many still respect their personal doctor but distrust the machine behind them. Other studies, surveys, and publications reveal more of the declining trust that exists among the public in the medical industry complex.
As time marches on past those early days of COVID, what is revealed is a widening gap between trust and truth. Promises of certainty gave way to shifting narratives, conflicting mandates, and data that often contradicted itself. What was once presented as unquestionable science now appears, in hindsight, to have been a mixture of urgency, politics, and profit. The science should have always been questioned. For many, the revelation is sobering: the institutions they leaned on for clarity and protection were not always guided by transparency or consistency, but by competing agendas that left the public confused, divided, and wary.
The Economic Trap: Who Really Pays the Bill?
Here’s the paradox: we think insurance “pays the bill.” But ultimately, the individual pays.
Individuals do so through premiums, co-pays, and deductibles; through lost autonomy—being forced into the narrow channels of what insurance will cover; through bankruptcy if uninsured (two-thirds of U.S. bankruptcies are tied to medical expenses).
Most medical decisions are predicated on money. A doctor may recommend one treatment plan not because it’s best, but because it’s what insurance will reimburse. That’s not health—it’s economics masquerading as care. The uncomfortable truth is that money dictates care far more often than anyone wants to admit.
And when patients attempt independence—choosing integrative, nutritional, or natural approaches—insurance doesn’t just fail to help. It feels like a punishment. Out-of-pocket costs lock most people out of alternatives, leaving them trapped in the industrial pipeline.
What gets left out in this model is the very person most affected—the individual. Patients are rarely empowered to do their own research, weigh their own options, or make independent choices about their bodies. The system is not conducive to such autonomy. Instead, there is a cultural expectation that we should “do what the doctor ordered” with no further questions asked. To question, to research, or to choose differently is often seen as suspect, even irresponsible.
There was a narrative made most clear in a 2020 Forbes article: “You Must Not ‘Do Your Own Research’ When It Comes To Science.” There might be some legitimacy at micro levels in this kind of advice, but pull in the diminished trust factor that exists in the culture and such advice comes across as dismissive and paternalistic; “we’ll make the decisions for you and for your own good; never mind your autonomy or your agency.” This fuels suspicion rather than building confidence. When institutions are already struggling with credibility, telling people not to inquire for themselves sounds less like protecting them from error and more like protecting the system from scrutiny.
There is something deeply wrong with this assumption. Especially when the reality is that within the current medical paradigm, disease and infirmity are rarely cured. They are managed. Patients are caught in a cycle: symptoms muted, causes ignored, new complications emerging, and more prescriptions required.
For many, the trap is even tighter. Even the smallest step toward independence—pursuing natural remedies, nutritional technologies, or self-care practices—comes with cultural stigma and ever-present financial penalty. Outside the insurance umbrella, these choices are labeled “alternative” and often dismissed; and if not dismissed, treated as tolerable. Worse, they are paid out of pocket, making them inaccessible to all but the most financially free. The result is a culture of forced dependence. If you have medical insurance, you are locked into the system. If you don’t, the specter of bankruptcy looms over any significant medical event.
Many people without medical insurance have made an eye-opening discovery: paying cash can actually work in their favor. When they offer a negotiated cash payment, they’re often surprised at how willing doctors and clinics are to provide significant discounts. For many providers, accepting cash is far simpler and faster than navigating the burdensome paperwork and delays of insurance reimbursement. While not true in every situation, many who choose this approach discover that their overall healthcare costs—when paying directly in cash—end up being far lower than the combined expense of insurance premiums and co-pays.
The Rise (and Risks) of Patient Advocacy
The cracks in the system have given rise to patient advocacy organizations and services. The global patient advocacy solutions market is projected to exceed $1 billion by 2025, growing at over 10% annually. Startups like Solace have raised venture capital to offer advocacy services, guiding patients through the labyrinth of hospitals and insurance. Many hospitals now employ “advocates” or “navigators.”
But here lies a danger: conflict of interest. If the advocate works for the hospital, they answer to the hospital. If they work for the insurer, they answer to the insurer. Only independent advocates truly answer to the patient—but these are rarely covered by insurance and often out of reach financially.
True advocacy remains outside the system precisely because independence threatens institutional control.
When advocacy is institutionalized inside the same system that creates the problems (insurance bureaucracy, hospital billing, treatment decisions), patients may feel like the “advocate” is more of a liaison than a protector. The appearance of advocacy can function as customer-service optics rather than true empowerment. This is why many families who can afford it (and many cannot) now hire independent advocates—nurses, social workers, or trained professionals who work only for them.
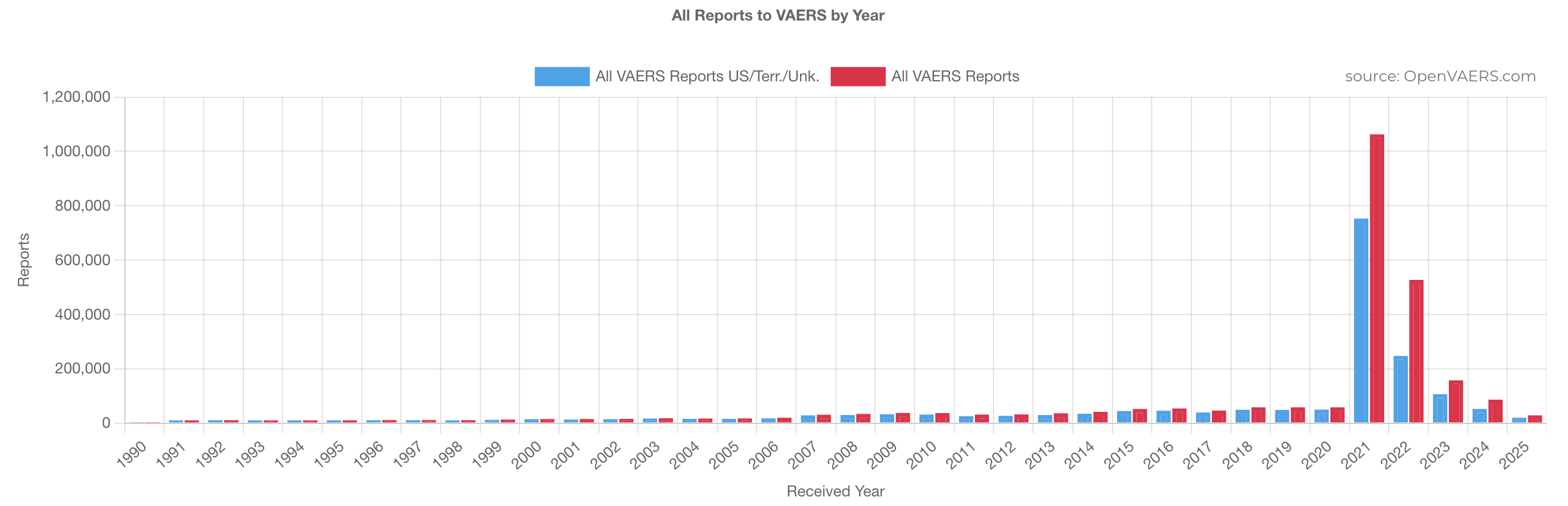
The Evidence of Underreporting: VAERS as a Case Study
The Vaccine Adverse Event Reporting System (VAERS) is a microcosm of the larger issue: underreporting and dismissal.
VAERS was created in 1990 as a trade-off. Once vaccine manufacturers were shielded from lawsuits by the 1986 National Childhood Vaccine Injury Act, there had to be some mechanism to monitor safety and preserve public trust. On paper, it looked like accountability. In practice, it remained largely invisible. Ask the average parent about VAERS, and most had never heard of it. For decades, this supposed safeguard sat in obscurity—until 2021, when COVID vaccines and boosters triggered a surge of reports that brought it into the public square for the first time. Suddenly, headlines carried a name that had once been a best-kept secret. Even now, many remain unaware it exists.
VAERS is often dismissed as a “passive” system where anyone can file a report, but such framing ignores important realities. Submitting a report is not user-friendly—it is time-consuming, technical, and discouraging by design. Which means that those who persist likely experienced something serious enough to justify the effort. Verification on the back end is indeed limited, but the fact remains: thousands of individuals went through the difficulty of documenting injurious events. However, as Aaron Siri mentions in his book, Vaccines, Amen, “the vast majority of reports come from pharma companies, health care providers, and state immunization programs.”
And the data is sobering. The Harvard Pilgrim study (2007–2010) revealed that VAERS may capture fewer than 1% of actual adverse events. In the case of serious vaccine injuries, Harvard estimated only 1% to 13% were captured. Even at the high end, this represents massive underreporting, suggesting that what we see in VAERS is not an inflated picture but a fraction of the reality—an “iceberg” effect where most of the damage remains hidden beneath the surface as not reported.
This pattern mirrors the broader medical system, where adverse drug effects, hospital infections, and iatrogenic harm are consistently minimized, under-coded, or ignored. Transparency is inconvenient when trust—and billions of dollars—are on the line.
The landmark studies by Barbara Starfield (2000) and Martin Makary (2016) already opened the conversation, showing that the medical industry complex itself is a leading cause of death. VAERS statistics add fuel to that fire by revealing streams of vaccine adverse event reports, and if they align with Harvard’s findings of underreporting, reveal a huge problem is happening right under our noses. Together, they suggest that iatrogenic mortality is consistently undercounted—whether from drugs, procedures, or vaccines.
The Shield of 1986
What looms over all vaccine discussions is the 1986 law that prevents lawsuits, shielding manufacturers from liability and transferring the burden of compensation to a federal program that cannot possibly be well funded enough to cover the claims. While this was intended to preserve vaccine supply during a wave of lawsuits, the result has been a system where accountability is blurred, trust is strained, and injured individuals must fight bureaucracy for limited compensation instead of seeking complete justice in open court.
Think about it—what other industry enjoys such immunity? Imagine an auto manufacturer protected from lawsuits if defective cars caused deaths, or a food company immune if their products made people sick. Wouldn’t such immunity demand an even higher standard of transparency and independent or third-party research? Instead, the opposite has occurred. Liability has been removed, and with it, much of the incentive to conduct rigorous, comparative studies that might cast doubt on product safety.
To get on the right track, we need to repeal the following laws:
- Bayh–Dole (1980) ensured that ownership and profit from medical innovation could flow to private entities, even though the research was funded by the public.
- National Childhood Vaccine Injury Act (1986) removed the liability risk for one of the most profitable and sensitive sectors—vaccines—placing the burden of harm on the public.
- PREP Act (2005) extended that shield to almost everything used in a declared emergency, from antivirals to masks to experimental vaccines.
The result is a three-layered shield: Until these laws are repealed the public funds the science; private companies own and profit; and legal immunity ensures profits are protected, even when harms occur.
The system is upside down. The incentives tilt heavily toward commercialization, not caution. Accountability is blunted at every level—first by shifting ownership, then by removing liability, and finally by granting blanket immunity in emergencies. Trust, once assumed, is now eroding because the safeguards for the public are thinner than the protections for the industry.
Privilege and Power: Pharma in the Public Square
Alongside legal immunity, pharmaceutical companies also enjoy another privilege: the ability to directly advertise their products to the public. This creates an inherent conflict of interest for network news organizations, which rely heavily on drug company ad revenue. Only two nations on earth allow such advertising—the United States and New Zealand. The result is a media environment where critical questions about safety are muted, while glowing advertisements flood the airwaves. Pharmaceutical companies must stand on their own merit with accompanying scientific studies and statistics gathered by third-party researchers who verify drug effectiveness or lack thereof. And the $22 billion of media advertising must stop.
And even with their immunity, pharmaceutical companies as a whole have hardly stayed out of court for non-vaccine issues. Between 1991 and 2021 alone, the industry faced 482 settlements, paying out a staggering $62.3 billion in financial penalties. $46.9 billion is considered civil penalties and $15.5 billion is classified as criminal. Legal exposure is constant and a status quo reality of the pharmaceutical industry—except, of course, when it comes to vaccines.
The Common-Sense Question No One Asked
Into this backdrop comes the recent Henry Ford Health System study (revealed September 2025). Despite critiques of methodology, controversy, and attempts at dismissal, the study points back to a simple, common-sense question: why has a straightforward comparison of vaccinated versus unvaccinated populations not been done—publicly and transparently—long before now?
Vaccines are one of the most widely used medical products in history, administered to millions of children and adults worldwide. Logic driven by strong ethic would suggest that a straightforward comparison of vaccinated versus unvaccinated populations — health outcomes, chronic conditions, long-term trajectories — would be priority research, conducted early and often. If the goal is public trust, hard comparative data should be the foundation. Especially when the public has no legal recourse in the event of vaccine injury.
Yes, this Henry Ford study was actually performed before 2020 with a focus on over 18,000 children born between 2000 and 2016, but the results were not revealed until September 2025, allegedly because the research leaned in a direction “unfavorable” to the accepted vaccine narrative. If true, that suppression itself is more damaging to public trust than any set of awkward numbers could ever be. Within a short period of time from its exposure at a congressional hearing where Senator Ron Johnson of Wisconsin provided a public stage for its data, this Henry Ford study had critics quickly point to its controversies, critiques, and methodological weaknesses. But all this attention to a single study again points back to simple, almost self-evident questions: why has such a comparison not been made, publicly and transparently, long before now? And why all the energy to discount it? Wouldn’t it make sense to carry out even more rigorous follow-up studies like this each year, using data from multiple health systems across the country—and even globally—to strengthen and verify the findings?
A Business Model Without Fear
Here lies the heart of the issue. Vaccine manufacturers operate under a model most businesses could only dream of: manufacture a product, distribute it globally, even mandate its use, reap enormous profit, heavily fund public and legacy news organizations who will fulfill your wishes—yet face no threat of lawsuits if harm occurs.
But for the public, this is a nightmare. The absence of liability, paired with the absence of transparent comparative studies, creates a void of accountability. If confidence in safety is so absolute, why the reluctance to put that confidence to the test? Why suppress, delay, or dismiss the very studies that could strengthen public trust? Moreover, if vaccines are truly delivering better health outcomes for the broader population, one would expect those supporting this claim to eagerly promote and publish such studies without delay.
The silence—and worse, the censorship—speaks volumes.
Beyond the Ledger: Health as a Living Condition
Modern health has been reduced to something transactional, processed, and packaged like a product on a shelf. Health is defined not by wholeness or resilience, but by diagnostic codes that fit neatly into insurance claim forms. The body becomes a series of billable events—each symptom reduced to an ICD-10 code, each treatment defined by a procedure number. What cannot be coded often cannot be counted, and what cannot be counted rarely gets addressed. Decisions about care are increasingly dictated not by the patient or even the physician, but by what an insurance company will cover. Treatments are approved or denied based on actuarial tables and cost-benefit spreadsheets, rather than what will actually restore health. In this model, insurance does not insure wellness; it insures conformity to what it will pay for.
Even the vocabulary of healing has been monopolized. The word cure is reserved by regulatory decree for conventional medicine, while natural or nutritional interventions are silenced, even when evidence points to efficacy. This linguistic control is not trivial—it shapes perception, policy, and permission. It tells the public what is “legitimate” and what must be dismissed, regardless of outcomes.
Success in this system is often defined by patient compliance: did you take the medication, follow the protocol, keep the appointments? Rarely is success measured by restored vitality, resilience, or long-term flourishing. The patient who complies but remains chronically unwell is still considered a success story on paper.
Reclaiming Health
But health is not a commodity to be rationed, coded, or linguistically fenced in. Health is a living condition—something to be cultivated, restored, and fully lived. It is not about mere survival or symptom management; it is about resilience, creativity, energy, and freedom.
This is where reclamation begins. Reclamation is not denial of medicine’s place; it is restoration of balance. It affirms that conventional medicine has tremendous value in moments of crisis—when the body is broken, bleeding, or failing. Trauma care, surgery, and acute intervention are areas where modern medicine shines. But beyond crisis, it carries a heavy burden of proof to show it can deliver patients to a place of sustained wellness and restored vitality, rather than managed decline.
What has been neglected—often suppressed—are the domains of nutritional science, prevention, and immune intelligence. These are not “alternative” or optional add-ons; they are essential companions to medicine. They address root causes, not just symptoms. They equip the body to resist disease, recover more fully, and thrive over the long term.
The future must be one of integration, not exclusivity. Medicine and nutrition, surgery and prevention, pharmaceuticals and lifestyle interventions can stand side by side—not in hierarchy, but as co-helpers. Only then can we move from a system designed to manage decline into one designed to cultivate life and wellness.
The vision of integration is offered in the previous paragraph with some reluctance. I am wary of propping up institutions under the guise of superficial diplomacy to keep the peace. Cooperation across disciplines is not only possible but in some cases necessary — yet it cannot come at the expense of individual autonomy. Too often, ‘standards of care’ are accepted as unquestionable, even when they are flawed from the start or cannot pass the test of efficacy or of time. True collaboration must allow for these standards to be examined, challenged, and refined. Input from every corner — medicine, nutrition, prevention, and the individual themselves — can be honored, but it’s likely that in some situations a certain discipline must sit this one out, because certain principles are violated or the sovereign individual vetoes a given protocol. The highest regard belongs not to institutional protocols, but to the freedom and responsibility of each person to make decisions for their own health. Where they get their education to make their decisions is totally up to them.
The Technology of Hope
Reform, Not Rebellion
I hope to rise in this context as a contributor in the field of unique nutritional wisdom—not rebellion against medicine, but reform of the entire framework through which health is understood. It is not about tearing down hospitals or replacing physicians, but about restoring balance and bringing neglected, proven science back into the center of human flourishing. And to encourage it in all disciplines and corners of the globe.
To be clear, my team markets products, ideas, and nutritional technologies. We’re upfront that The Hope Movement is not just a philosophy or abstract advocacy—it is also sustained by products and innovations that we believe are unique, efficacious, impactful, and compelling.
Acemannan: A Category-Defining Molecule
At the core stands Acemannan, the most validated natural polysaccharide ever studied. Backed by over 700 peer-reviewed studies, more than $100 million in research investment, and 130+ patents, Acemannan has earned its place as the crown jewel of immune modulation. This is not folklore dressed in modern language. This is empirical science demonstrating that the body can be guided back into balance, resilience, and repair when given the right molecular tools.
Second-Generation Trade-Secret Protection
The story doesn’t stop with discovery. The Hope Movement carries an exclusive, second-generation form of stabilized Acemannan that is both more bioavailable and more potent. Protected not by patents but by trade secret, this evolution ensures both exclusivity and integrity. It is stronger, safer, and reserved for the mission we steward. This is not a repeat of the past; it is a leap forward, one that only the Hope Movement can deliver.
Stacked Synergy: More Than the Sum of Its Parts
But Acemannan is only the beginning. The Hope Movement has gathered a suite of pioneering technologies designed not merely to stand alone, but to amplify one another in the human body. Together, they:
• Restore gut integrity, where over 70% of the immune system resides.
• Reduce chronic inflammation, the silent driver behind most modern diseases.
• Strengthen cognitive resilience, protecting the brain against decline.
• Fuel cellular energy, unlocking vitality at the mitochondrial level.
This is a system of technologies that function like an orchestra, where each instrument is powerful, but together they create symphonies of wellness impossible through isolated interventions. Though there are great technologies and modalities in the world, we stand by the value of our technologies and won’t pretend otherwise.
Social Business 3.0: Science Meets Purpose
What truly sets the Hope Movement apart is not only its science but its model. We call it Social Business 3.0—a new paradigm where every purchase fuels a greater purpose. For every product consumed, life-saving nutrition is delivered to vulnerable children across the globe. Profit is no longer an end in itself, but a vehicle for restoring lives, families, and futures. This is not charity; it is sustainable, scalable, purpose-driven commerce.
Nutrition 2.0: Beyond Managed Decline
This is not healthcare nutrition as usual. The Hope Movement offers Nutrition 2.0—a future where people no longer wait for symptoms to dictate their lives. Instead, they reclaim vitality at the cellular level: building resilience, preventing decline, and living not in managed sickness but in active, thriving health.
In this reform, medicine retains its rightful place in emergencies and acute interventions. But alongside it stands an empowered vision of human wellness, where people are not reduced to codes, compliance, or commodities, but are invited to reclaim their health as a living condition to be cultivated and shared.
This is the balance we seek to restore. This is reclamation. This is the Hope Movement.
Why the System Resists (and Why People Must Demand Change)
If the evidence is compelling, the science is validated, and the need is urgent, then why is reform resisted? The answer lies not in a lack of proof but in the deeply entrenched interests of the system itself.
Economic Self-Interest
The medical industry complex is tied into a financial ecosystem worth trillions. Chronic disease management is its lifeblood—an endless stream of office visits, prescriptions, and procedures. If diseases like diabetes, heart disease, or autoimmune conditions were truly reversed at scale, billions in annual revenue would evaporate. From pharmaceutical companies to insurers to hospital systems, too many stakeholders have built their fortunes on managing symptoms rather than resolving causes. To expect this system to dismantle its own business model voluntarily or even submit to reasonable reform is to misunderstand its survival instinct.
Intellectual Pride
Doctors and specialists invest a decade or more in training, with immense personal and financial sacrifice. Their identity and authority are bound to the paradigm in which they were educated. To admit that nutritional science and immune modulation and a hundred other ideas or modalities may hold answers they were never taught is not just humbling—it is destabilizing. It requires acknowledging blind spots, even errors. The natural human response to such cognitive dissonance is defensiveness. Thus, newly uncovered truths are often resisted not because they lack merit, but because they wound pride.
Institutional Inertia
Hospitals, universities, and medical associations are vast bureaucracies. They thrive on standardization and predictability, not disruption. Every new model threatens established protocols, accreditation processes, and funding streams. Bureaucracies do not pivot easily; they prefer to reinforce what already exists. This inertia slows or stalls even the most promising reforms, leaving patients to suffer while institutions preserve the status quo.
Legal Fear
The regulatory climate compounds the resistance. Doctors are bound by “standard of care” protocols, not by innovation, especially not the innovation their patients are willing to research and try or glean from professionals outside the system. To deviate—even when convinced a better approach exists—exposes them to lawsuits, licensing risks, or professional censure. The irony is striking: a doctor may be punished for seeking to restore a patient to full health if that path falls outside the sanctioned menu of treatments. Fear of legal reprisal becomes a leash, keeping many professionals in line with a model they privately question. The recent COVID pandemic, its accompanying protocols, and jabs found much of its forward movement not in common sense and research-backed science but among the best-paid medical professionals who had too much to lose by not cooperating with federal mandates.
Progress Rarely Comes from the Old Order
History shows that revolutions in thought and practice rarely emerge from those most invested in the old order. Penicillin was resisted. Handwashing in hospitals was ridiculed. And yet, reform prevailed—because courageous reformers valued truth and efficacy above self-preservation. To this day, reform still stands at the door knocking, challenging truth lovers to embrace the responsibility to bring answers to the unanswered questions. New discussions are underway about terrain theory vs germ theory; fresh discussions about penicillin and pharmaceutically-expanded antibiotics; viruses not yet isolated; and vaccines embarrassingly and shamefully short on safety studies.
The same is true now. If the system resists, then the people must demand change. Families, communities, and entrepreneurs must refuse to accept “managed decline” as the definition of health. They must insist on balance, transparency, and the freedom to choose — whether that means integrating restorative approaches with conventional medicine, or, in many cases, pursuing a path apart from conventional medicine altogether. The burden of proof has shifted, and the people must no longer tolerate dismissal of evidence that points toward a more hopeful, more empowered health and wellness future.